
This week we ran the inaugural Resuscitology UK course here in Virchester (Ed – everyone knows you mean Manchester 😉 ). Resuscitology UK aims to improve the way we think about resuscitation practice through case discussion, analysis and expert debate. The course has run several times in Australia, with this being the first in Europe.
Candidates submit cases in advance of the course and we select those that are likely to be challenging and which allow the faculty to explore the core learning outcomes for the course. An analysis from past cases submitted suggests that there are common themes for us all. Paediatrics, Obstetrics, Human Factors, Decision making, Complexity, Scene management and Airway are the areas where it seems our learners want to explore, and in truth those are the areas we want to explore too.
The case based format means that there is always some variation in content and learning about specific clinical issues, but underpinning the course are the principles of case analysis as designed and championed by Cliff Reid and the rest of the Resuscitology UK team.
STEPS analysis1
This is a way of analysing cases to decide why things happen and not just to describe what happens. When we look back at events breaking down the analysis into the components listed below allows to understand how the different parts can perform, but also how they interact with one another to produce the patient outcome

You will of course realise that the STEPS process is remarkably similar the same as the Zero Point Survey which we also champion on the course. This makes perfect sense if you think about it as the ZPS is designed to mitigate poor outcomes and promote excellence in resuscitation teams. It therefore follows that the analysis of cases can and should use the same model. Read more about the origin and development of the STEPS system on Cliff Reid’s blog here.
GPAS analysis2
GPAS is an additional way of analysing cases to describe why a plan may have appeared to be satisfactory when analysed through STEPS, but where for some reason the plan did not (or perhaps did) work. GPAS stands for Goals, Plan, Actions and Skills.
Goal (what are we trying to achieve)
Strategy, or Plan (what’s our plan to get there?)
Tactics, or Actions (what procedures will be required to execute the plan)
And, at more granular level: If we’re failing at the procedural level, the components of procedures, namely Skills & Microskills.
So, as we zoom in from macro to micro in setting the clinical trajectory, we can look at Goals, Plan, Actions, and Skills:

Combining STEPS and GPAS
In Cliff’s words on the resus.me website
These models may prove helpful as a means of dissecting a case in a structured way. Put simply, STEPS offers a structure for identifying efficiency improvements (“doing things right”) and GPAS can help us assess effectiveness (“doing the right things”).
Another way of looking at it is that STEPS provides the components of a resus at any point in time, and GPAS defines the trajectory: where the resus is going and how to get there.
So what did we learn in Manchester?
We were hugely fortunate to have Nick Smith on the team who produced visual summaries for the sessions and which are reproduced here. Clearly the nuances and details of the cases are not for public discussion on the blog, (Ed – you’ll need to come on the course for that), but these clearly demonstrate how the entire group explored some really challenging and emotive cases.
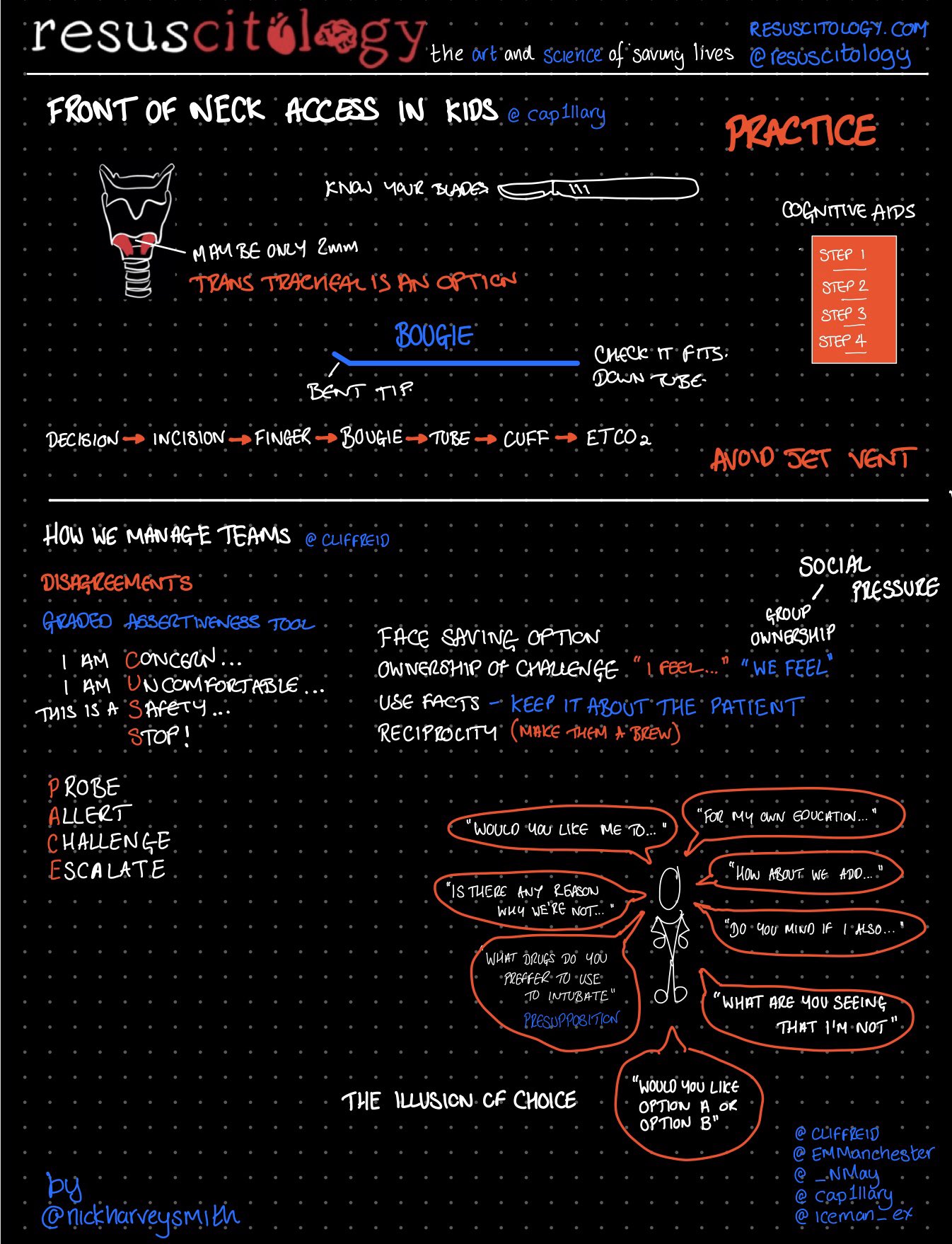
Airway session led by @Cap1llary
Main themes in this session were airway management in small children, choking procedures, decision making in partial obstruction. This session introduced us to some of Cliff’s mind tricks of communication such as illusion of choice and pre-supposition statements (amazing and will be used in Virchester soon).
Case discussed: Complex management of obstructed paediatric airway.
Cardiac Arrest session with @iceman_ex
Case discussed: Young cardiac arrest with possible toxicological cause. Scene management, forward thinking situational awareness and language use in resuscitation settings were all discussed. The Resuscitology UK attendees particularly liked the COACHED approach to defibrillation3. Something we’ve been teaching in Virchester insitu sim, but not widely done in UK.
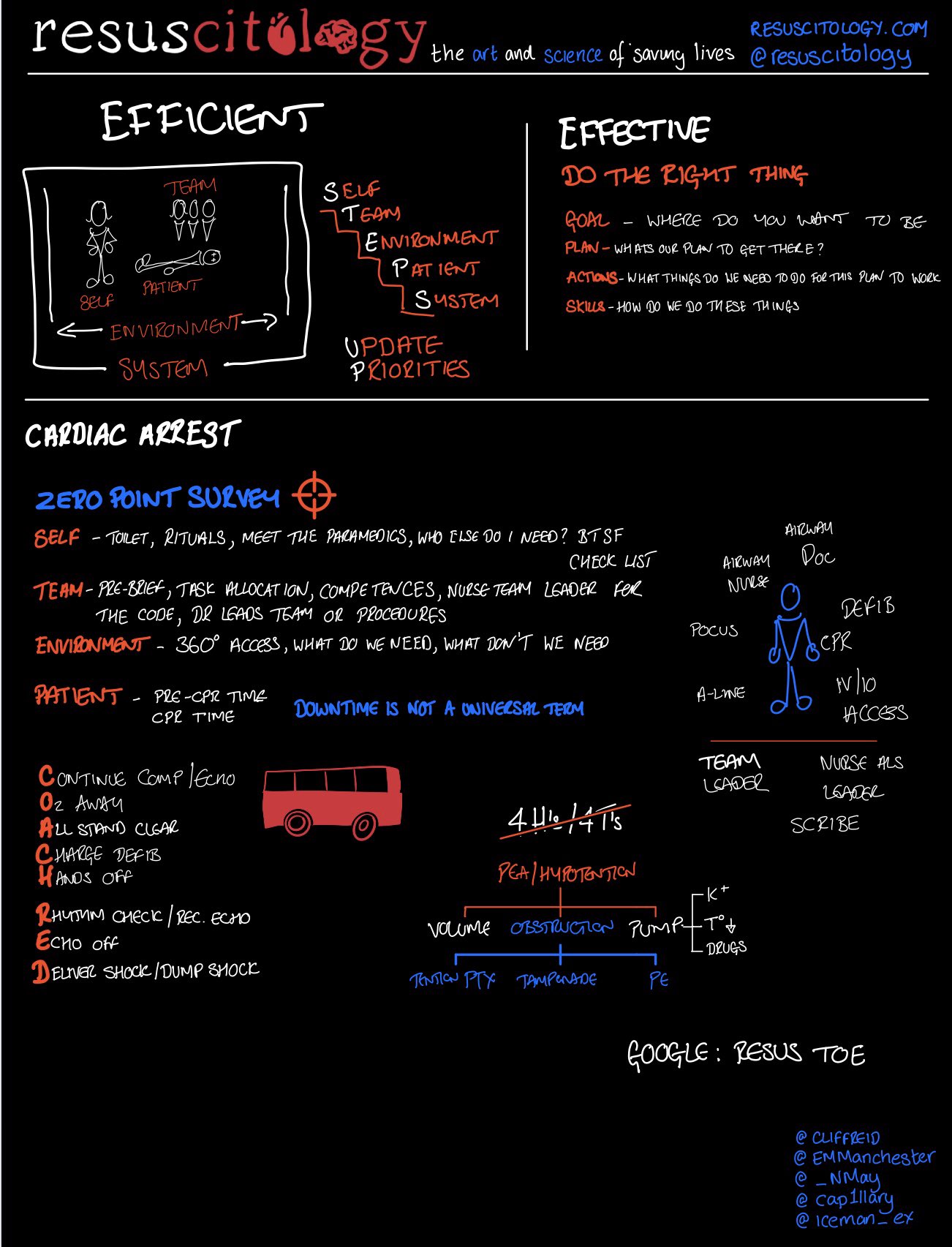
This session also embedded the STEPS approach and its linkage to the Zero Point Survey4.
Paediatric session led by @_nmay
Case discussed: hemorrhagic shock in baby. Focus on major haemorrhage protocols in children, IV/IO access and human factors in complex emergency

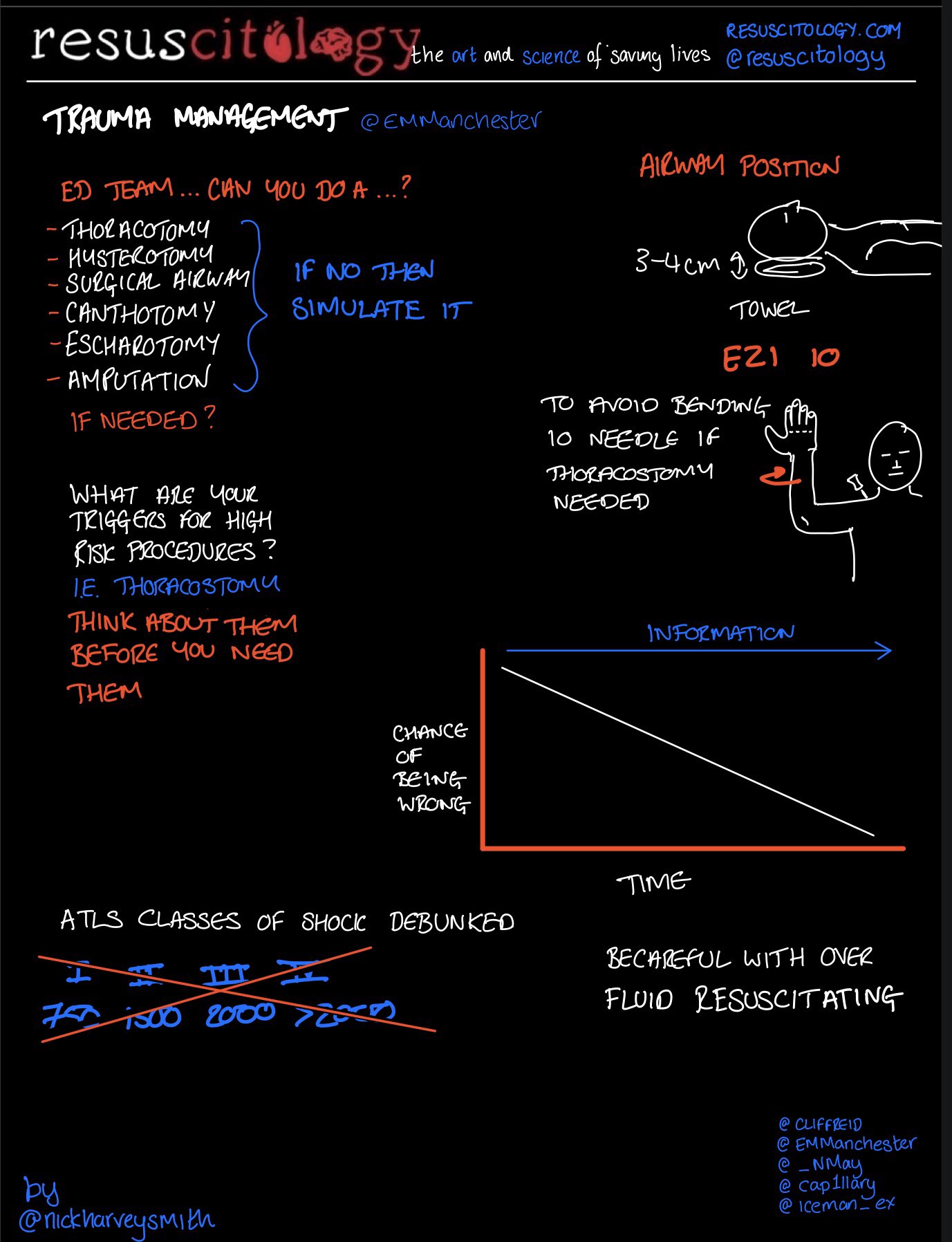
Trauma session led by @EMManchester
Case discussed: Resuscitative Hysterotomy5. Rare life and limb threatening procedures, complex team management and decision making were the main themes in this Resuscitology UK session
Wellness sessions with @cliffreid
There were arguably a few of these scattered through the cases, but also in a separate session led by Cliff. The concept of ikigai came up again as did evidence based strategies to improve your personal happiness and satisfaction with work.
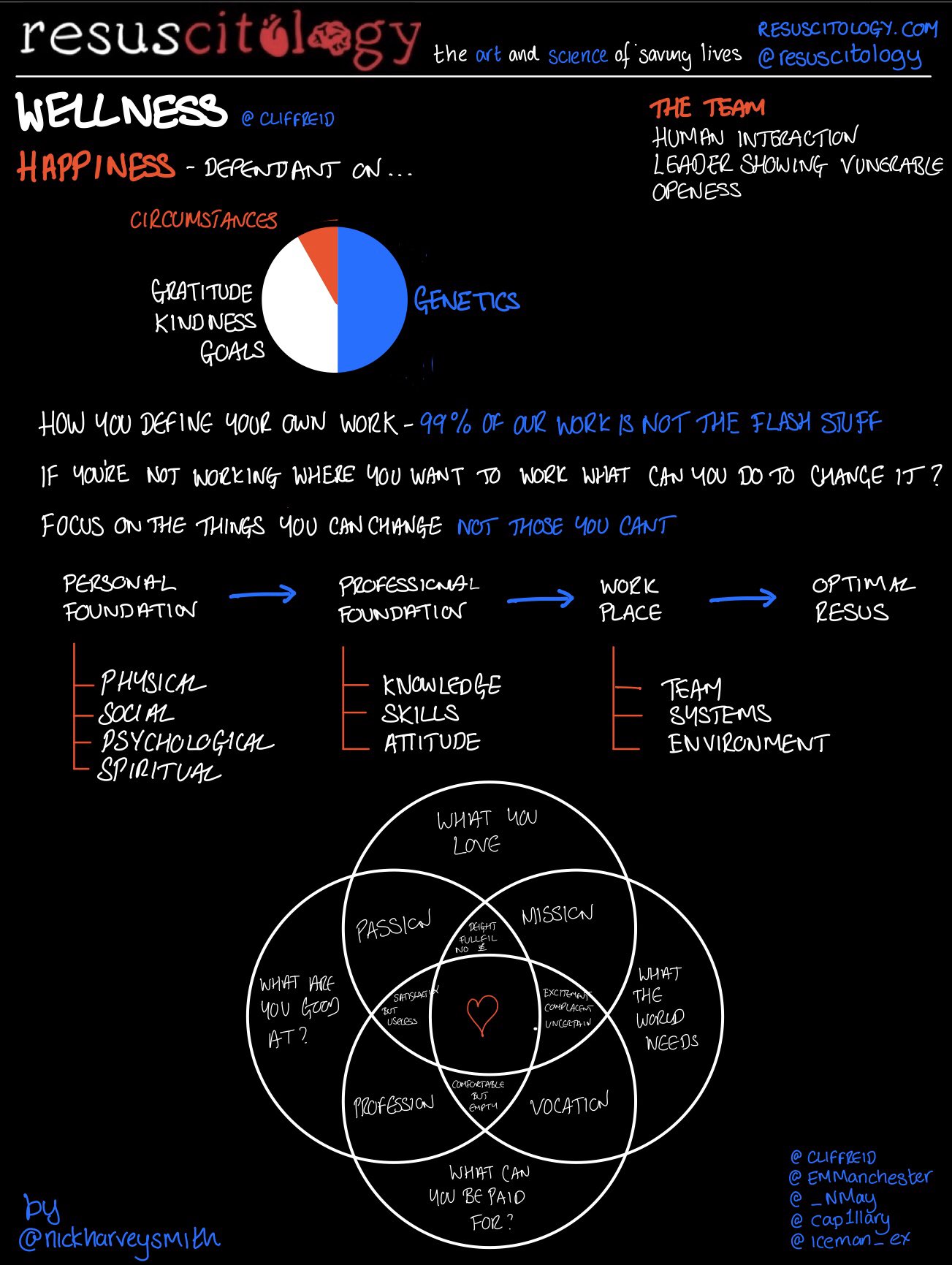
There was also further discussion of the use of language to advocate for ourselves and our patients. I’m pretty sure every one of us came away with communication skills that could dramatically change our working environments for the better.
Will the course run again in the UK?
Yes. We are aiming to do another Resuscitology UK course in May 2020. This will likely to be the two day version to allow more time to discuss cases, for the groups to bond and also for a few more games. We’ve not talked about the games here as you really need to experience them without prior knowledge to get the most out of them.
Finally it was a delight to get some fantastic positive feedback in person and online after the course. We will be following everyone up from the course with a postcard detailing what you learned in a few months time (Ed – this is the write your own postcard and we post it back to you as a reminder technique we started at #stemlynsLIVE in 2018).
- 1.Reid C. Analysing difficult resus cases part 1. Resus.me. https://resus.me/analysing-resus-1/. Published 2018. Accessed 2019.
- 2.Reid C. Analysing difficult resus cases part 2. Resus.me. https://resus.me/analysing-difficult-resuscitation-cases-2/. Published 2018. Accessed 2019.
- 3.Coggins A, Nottingham C, Chin M, et al. A prospective evaluation of the ‘C.O.A.C.H.E.D.’ cognitive aid for emergency defibrillation. Australasian Emergency Care. August 2018:81-86. doi:10.1016/j.auec.2018.08.002
- 4.Reid C, Brindley P, Hicks C, et al. Zero point survey: a multidisciplinary idea to STEP UP resuscitation effectiveness. Clin Exp Emerg Med. September 2018:139-143. doi:10.15441/ceem.17.269
- 5.Carley S. Peri-mortem C-section and hysterotomy. St Emlyn’s. https://www.stemlynsblog.org/peri-mortem-c-section-at-st-emlyns/. Published 2013. Accessed 2019.