
This week we are reviewing a paper on the accuracy of pulse oximetry in patients being assessed for ECMO. This is an interesting group as they represent and extremely unwell group of patients where small changes in measured SaO2 might lead to significant changes in management.
This is not the first paper to look at the question of skin pigmentation and pulse oximetry. Although there is a large body of work going back decades that have identified this as a potential issue I will personally admit that it is not something that I was aware of until the publication of an observational study from Michigan last year. That paper can be read here. It is, in my opinion, an essential read for anyone who uses pulse oximetry in emergency settings.
Since then there has also been a useful document published by the NHS Race and Health Observatory containing recommendations for how we might adapt this information. That document highlights the importance of identifying patients who may have silent hypoxia, i.e. significant hypoxia without other obvious signs of hypoxia such as tachycardia, tachypnoea etc. That’s something we’ve seen a lot of in COVID19 infections, but also something that we are often concerned about in patients with other conditions, in this case sickle cell disease with occult pulmonary involvement springs to mind as an area of potential concern.
You should also read this document from the Intensive Care Society outlining next steps in the UK.
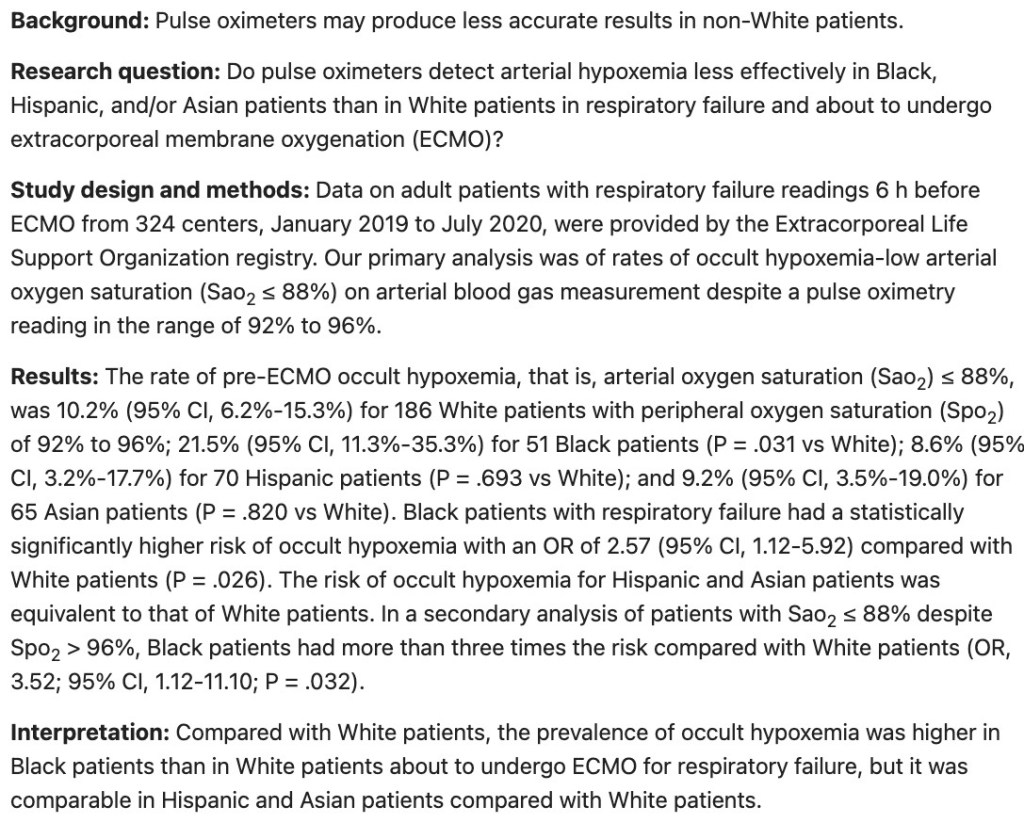
The abstract of the paper is shown below, but as always we strongly recommend that you read the full paper for yourself. Please also read the links in the references to gain a broad understanding of the issues.

What kind of paper is this?
This is a retrospective review of registry data. Such studies can be useful if the data collected into them is of high quality, but in general we are relatively cautious about interpreting the results as the data is not collected in a focused and/or prospective manner. It is therefore more likely to contain inaccuracies and bias. However, they can often be useful in bringing attention to an issue that warrants further investigation and they can often reveal data trends quickly in circumstances where the prospective collection of data would be lengthy or difficult.
Who has been studied here?
This paper focuses on those patients who were being assessed for ECMO. All the patients had reported arterial gases and oxygen saturations within 6 hours of staring ECMO. Where multiple results were obtained the ones closest to the onset of ECMO were chosen. The data was extracted from the notes by a data manager.
Race was defined using standard US definitions. It’s worth noting that definitions of race may vary between different health economies. For example, in the UK we do not routinely define a ‘Hispanic’ population as they did in this paper. Such different classifications may hinder the generalisability of the findings. In this paper the groupings were as follows; Asian, Black, Hispanic, Middle Eastern or North African,Native American, Native Pacific Islander, Multiple, Other, Unknown, and White. So clearly very different to the categories we use in the UK.
The authors did perform a sample size calculation which is always a little tricky to do in studies like this. It is well described and seems reasonable with the number of patients required estimated to be >400. Within the database there were 4 racial and ethnic groups that reached this threshold; White, Black, Hispanic and Asian. Other groups presumably had too few cases for analysis.
What did they do?
Simply put they compared the SaO2 values as obtained through non-invasive pulse oximetry with that obtained from the arterial blood gas.
Occult hypoxemia was defined as SaO2 <88% despite SpO2 between 92% and 96%.
White patients were then used as a reference standard to compare differences between the racial/ethnic groups.
What are the main findings?
In the group of 372 patients who had an SpO2 of 92-96% the incidence of occult hypoxaemia was as follows.
- White 19 of 186 pts (10.2%; 95% CI, 6.2%-15.3%)
- Black 11 of 51 pts (21.5%; 95% CI, 11.3%-35.3%)
- Hispanic 6 of 70 (8.6%; 95% CI, 3.2%-17.7%)
- Asian 6 of 65 (9.2%; 95% CI, 3.5%-19.0%)
So the big message here is the big difference between black patients and other racial groups.
The authors also performed a logistic regression on the data using White patients as the comparator. In that analysis Black patients had a statistically significantly higher risk of SaO2-defined occult hypoxemia (OR, 2.57; 95% CI, 1.12-5.92) as compared to White patients (p= 0.026).
Similar findings were observed in those patients with an SpO2>96%. Black patients with SpO2 >96% had a statistically significant higher risk of SaO2 <88% (OR, 3.52; 95% CI, 1.12-11.10) as compared to White patients (p= 0.032).
These findings, amongst a group of critically ill patients are in keeping with other studies in this area. This study is especially helpful in that it focuses on the most unwell patients in whom decisions about therapy may well be guided by measurement and trends in oxygen measurement.
Any concerns with the findings?
I think it’s pretty safe to say that there is a problem here with pulse oximetry and racial/ethnic groupings. However, if I cast a critical appraisal eye on the paper there are problems here, which are largely a result of the retrospective design.
We don’t know the type of pulse oximeter used, nor how it was used, nor how people were trained in its use. The study did not meet its target number of patients and some of the analyses are quite small in number as a result (leading to wider confidence intervals than we would like).
The study is in a very bespoke group of patients and so that limits the generalisability of this study in isolation which is why it is important to interpret this in light of other studies in the area.
It’s worth re-iterating the differences in definitions of racial/ethnic groups in the US and here. Of particular note is that Asian-American is predominantly Americans identifying as Chinese, Indian, and Filipino. That is not what we commonly define as British-Asians, which is more of an Indian sub-continent grouping. There are differences in skin pigmentation between these groups and I would personally love to see more data on the UK defined Asian population in this area. This differential in definitions is something that happens in a lot of papers and is always worth looking out for.
More than that, I’m uncomfortable with the definitions used here to divide the groups for analysis. I can understand why it has been done because this is a retrospective study. I can presume that the authors will only have had data on how patients self declared their race/ethnicity, but that’s really not the question here. The issue is one of skin pigmentation and whilst that is associated with those categories, it is a blunt tool that misses a whole lot of information about grades of skin pigmentation and whether that is indeed the factor (which it almost certainly is). So we need better research to look at what the technical issue is and not one that divide people up based on an answer to an entirely different question. In other words I want to know how skin pigmentation affects pulse oximetry, irrespective of how society chooses to classify people. We need to answer that alongside developing an understanding of and a solution(s) to challenging the systemic differences that we know exist in the assessment and management of different racial/ethnic groups.
What does this mean for us in practice?
Or rather, what does this paper and other papers in the area tell us? For me it highlights 2 things. Firstly that occult hypoxia can occur in all patients and is more common than I had previously suspected. Secondly, that this is a MUCH bigger concern in patients with more pigment in their skin. In practice this means that I will be lowering my threshold for doing an arterial blood gas in patients/conditions where there is a possibility of occult hypoxia, and especially so in those with pigmented skin. It also reinforces my practice that if I see a patient in whom it’s inevitable that I will be taking serial arterial blood gases then I place an arterial line.
We also need better research to help us understand why these differences occur and more importantly whether they can be mitigated. There is no doubt that pulse oximetry is an extremely useful clinical tool in emergency care and we should look for research that allows us to use it effectively in all patients. There are signs that this is starting to happen and I sincerely hope that we get some answers soon.
POST PUBLICATION: After publishing this blog the following tweet came through with links to an article in WIRED magazine that indicates that this is not only a known problem, but also one that has a solution.
vb
S
@EMManchester
POST PUBLICATION: After publishing this blog the following tweet came through with links to an article in WIRED magazine that indicates that this is not only a known problem, but also one that has a solution. I have also changed physiological in the text to technical as that more accurately describes where the issue lies.
Note on language and terminologies: I am aware of the complexities of describing research in this area. One of these complexities is in the use of acceptable terminologies. In this blog I refer to the concept of ‘racial/ethnic groups’. I have used the term ‘racial/ethnic groups’ as that was the term used in the paper. I appreciate that other writers may use different terminologies.
References and further reading
Racial Bias in Pulse Oximetry Measurement. https://www.nejm.org/doi/pdf/10.1056/NEJMc2029240?articleTools=true
NHS Race and Health Observatory Pulse oximetry and racial bias: Recommendations for national healthcare, regulatory and research bodies https://www.nhsrho.org/wp-content/uploads/2021/03/Pulse-oximetry-racial-bias-report.pdf
Racial Bias in Pulse Oximetry Measurement Among Patients About to Undergo Extracorporeal Membrane Oxygenation in 2019-2020. A Retrospective Cohort Study. https://journal.chestnet.org/article/S0012-3692(21)04065-4/fulltext
Intensive Care Society 2021. Pulse oximetry and ethnicity – the time to act is now. https://www.ics.ac.uk/Society/Policy_and_Communications/Articles/accuracy_of_pulse_oximetry
UK racial group categories. https://www.ethnicity-facts-figures.service.gov.uk/style-guide/ethnic-groups
Farkas J. PulmCrit – Dismantling the systemic racism of pulse oximetry https://emcrit.org/pulmcrit/racism-oximetry/
Salim Rezaie, “Racial Bias with Pulse Oximetry?”, REBEL EM blog, December 20, 2020. Available at: https://rebelem.com/racial-bias-with-pulse-oximetry/.
American Asian definition https://en.wikipedia.org/wiki/Asian_Americans
British Asian definition https://en.wikipedia.org/wiki/British_Asian