Picture the scene…
A 23 year old man has been brought in from home by ambulance with an acute onset of severe asthma associated with a rash.
Learning Objective
In this session we will cover the recognition and immediate treatment of anaphylaxis together with admission and discharge considerations.
RCEM Curriculum
CMP1 – Anaphylaxis
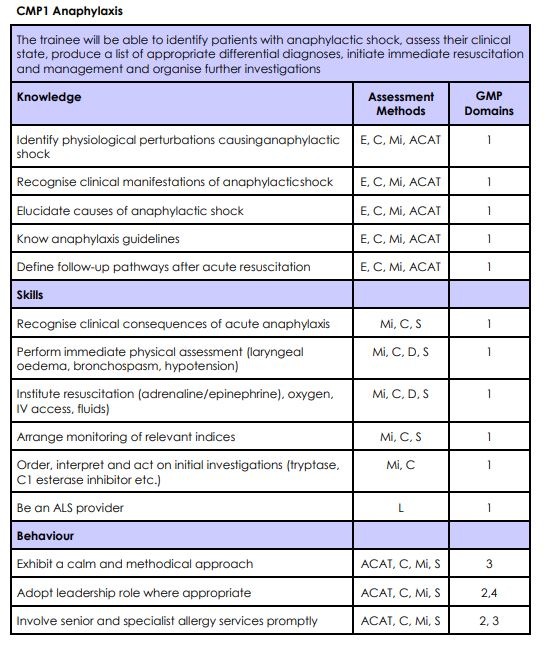
Task 1 – Knowledge
Read this comprehensive blog post from RCEM Learning.

The Anaphylaxis algorithm from the Resuscitation Council (UK) is an incredibly helpful summary.

Task 2 – Podcast
Listen to this podcast discussing the evidence around the treatment of Anaphylaxis
Task 3 – Discuss
This part of the teaching session should be lead by an experienced clinican. The cases provided are merely examples and if possible the learners should be encouraged to discuss patients they have seen in their clinical practice.
Case 1 – A 23 year old with asthma and a rash
A 23 year old man has been brought in from home by ambulance with an acute onset of severe asthma associated with a rash.
1, What are the defining features of an anaphylactic reaction?
An anaphylactic reaction involves an acute onset of rapidly progressive life threatening A (lip/tongue swelling, stridor), B (bronchospasm) and/or C (hypotension) problems, usually in association with skin or mucosal features (although these can be absent or subtle in 20% of cases).
2, What are the management priorities in a case of anaphylaxis?
As with any emergency, the ABC approach is a reasonable way to establish concerns. If anaphylaxis is suspected the treatment to finding any significant abnormality in the primary survey is to administer intramuscular adrenaline immediately.
Following adrenaline administration, oxygen, iv fluids and additional drugs such as salbutamol, antihistamines and steroids can be considered depending upon the specific features of the reaction and the initial response to adrenaline.
3, Why might a patient not respond to the initial dose of adrenaline?
Some reasons for a failure to respond to the initial dose of adrenaline include:
- A severe reaction – this initial dose may just be inadequate
- Ongoing allergen exposure – embedded stings, ingested foods, injected drugs
- Under dosing – ‘Adult’ Epipens deliver only 0.3mg of adrenaline
- Incorrect administration – in obese patients the dose may have been delivered subcutaneously
- Incorrect diagnosis – Asthma, Sepsis, ‘Panic’ Attacks, Angiodema.
3, What should one do if there is little or no response to the initial dose of adrenaline?
Whilst considering the options above, a second dose of intramuscular adrenaline after 5 minutes is recommended and can be delivered by any clinical responder.
If anaphylaxis is still the primary diagnosis and the life threatening features continue, titrated doses of diluted intravenous adrenaline followed by a continuous infusion may be required. This should only be done by experienced specialists. In cases of Cardiac Arrest thought to be due to Anaphylaxis, use the ‘normal’ 1:10,000 pre-filled adrenaline syringes.
Case 2 – A 47 year old with a reaction to nuts
A 47 year old woman has been brought to the ED following an anaphylactic reaction to nuts. She is known to have such reactions and tried to use her own Epipen as she became wheezy and dizzy, but it was broken. The paramedics noted the presence of wheeze and lip swelling on their arrival and administered adrenaline at the scene. On arrival at the hospital, her symptoms have now settled completely and the patient is keen to go home.
1, What is the recommended minimum observation period for patients following an anaphylactic reaction?
Observation for at least 6 hours is generally recommended although longer periods may be considered in those with more severe features.
2, What is a biphasic reaction, over what time period can it happen and how often does it occur?
A biphasic reaction is a recurrence of the initial anaphylactic symptoms without further allergen exposure.
It can happen at anytime from a few minutes after the initial episode to 3 days and estimates of their frequency run from less that 1% of cases through to as many as 20%!
3, What features of a case would make you more or less likely to support discharge from the ED after an anaphylactic reaction?
The admission or discharge of a patient should always be a joint decision with the patient.
Clinical features suggesting longer periods of observation would be appropriate include: a more severe reaction; slower response to adrenaline; use of a second dose of adrenaline; requirement for iv fluids; potential continued exposure to allergen (ie ingestion).
Patient features that may influence the decision would include: home circumstances; access to emergency services response; experience with anaphylaxis; ability to administer im adrenaline.
Before discharge, all patients should be aware of what symptoms to watch for; have in their hands (ie not just a prescription) two Epipens; and appropriate follow up ie GP or specialist OP review depending upon local resources.
Task 4 – Summary
Anaphylaxis is a life threatening allergic emergency causing rapid clinical deterioration. It can be caused by numerous different allergens, although specific exposure may not be obvious at initial presentation. Whilst a rash is usually present, in up to 20% of cases it is not.
The primary treatment is administration of adrenaline by the intramuscular route. In some resistant cases intravenous adrenaline may be administered by suitably trained critical care clinicians.
Admission/Discharge decisions are based on the severity of the initial presentation, the likelihood of a further reaction and the ability of the patient to manage another episodes. For those wishing to dive deeper in to the use of intravenous adrenaline, read this blog by Josh Farkas
Task 5 – Reflect
In order to embed today’s learning further, reflect on what you have learnt and record in your portfolio whether it has had any impact (or is expected to have any impact) on your performance and practice.
Was this a topic that you were confident you knew already? Which parts were new to you? Were there elements that you will use on your next clinical shift.
Dscuss this session with your colleagues – were there people who missed it who you can share the highlights with?