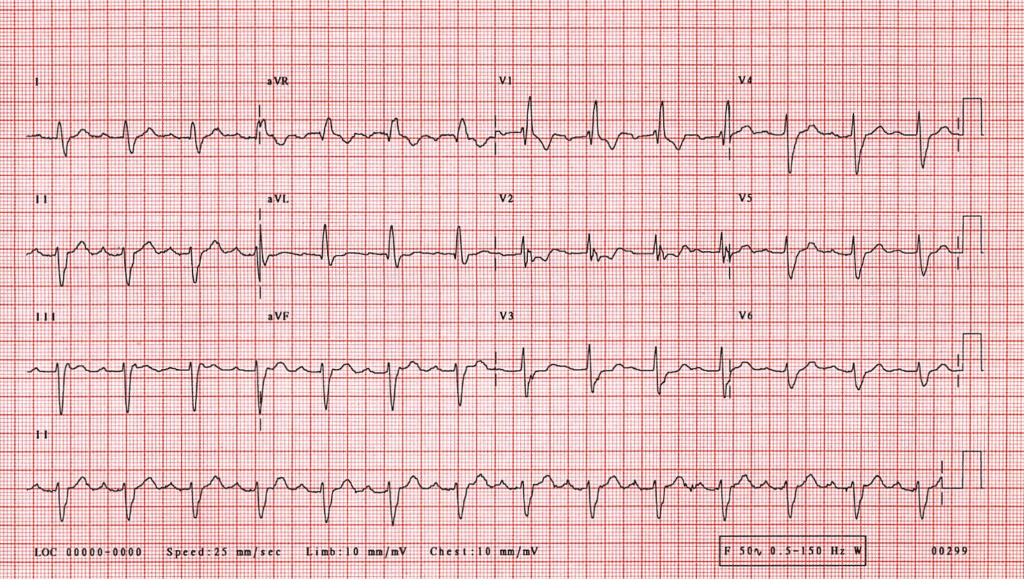
The ECG was recorded from a 62 year old man admitted through the accident and emergency department having collapsed in a supermarket.
ECG. Sinus rhythm is present. Each QRS complex is preceded by a P wave and no dropped beats are seen. The PR interval is constant but prolonged to .28 seconds indicating first degree AV block. There is left axis deviation. The QRS complexes are abnormally wide (at .16 seconds well above the upper limit of normal of .10 seconds). There is an rSR’ complex in lead VI showing a prominent secondary R wave. There are deep S waves in leads facing the left ventricle: I, aVL and V4 – V6. These are the appearances of right bundle branch block (RBBB).
Comment. In the presence of RBBB activation of the ventricle occurs entirely through the left bundle branch. This consists of two fascicles, an anterior superior one and a posterior inferior one, although the disdncdon is theoretical rather than anatomical.
In the presence of conduction block in the anterior division (left anterior hemiblock) activation of the left ventricle occurs from the posterior division, activation initially spreading towards the inferior surface of the heart (hence the R waves in leads II, III and aVF. The anterior left ventricular myocardium is activated later by spread of excitation distal to the site of block and this results in a vector directed to the left and superiorly. This results in S waves in the inferior leads (II, III and aVF) and left axis deviation.
Activation of the ventricular myocardium under normal circumstances therefore occurs through three fascicles: the right bundle and two divisions of the left bundle. If any two of these are blocked ‘bifascicular block’ is present but in practice the term is restricted to the combination of RBBB with either left anterior hemiblock or left posterior hemiblock. If both divisions of the left bundle are blocked complete left bundle branch block is present.
If all three fascicles were blocked no supraventricular impulse could be conducted to the ventricles and complete heart block would exist. The term trifascicular block is reserved for the combination of bifascicular block with a prolonged PR interval. The delay in conduction giving rise to the prolonged PR interval may be situated in any part of the AV node, bundle of His or left posterior fascicle, but intra cardiac studies often indicate that the problem lies in the remaining fascicle. Progression to complete heart block may occur which may initially be episodic.
Useful ECG Links
- St. Emlyn’s ECG Library.
- Life in the Fast Lane ECG Library
- Dr Steve Smith’s ECG blog
- Amal Mattu’s ECG weekly